This web page was produced as an assignment for Genetics 564, an undergraduate course at UW-Madison
Development of Polycystic Kidney Disease
Autosomal Dominant Polycystic Kidney Disease (ADPKD) is a genetic disorder characterized primarily by progressive cyst growth within kidneys, although it can be considered a multi-system disorder because many organs are ultimately affected [2]. The kidney cysts eventually replace much of the normal structure of kidneys, leading to reduced kidney function and ultimately renal failure [3]. The disease primarily manifests in adulthood, although there have been a clinically significant cases observed in infancy and childhood [4].
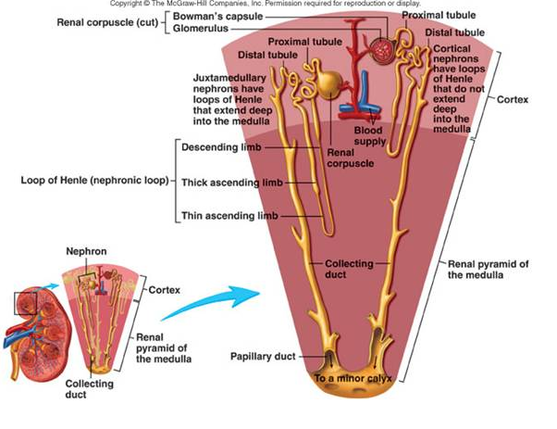
Cysts may develop from an increase in size of any part of the nephron, the functional unit of the kidney that produces urine and filters waste and excess substances from the kidney [5]. This graphic shows two nephrons side-by side.
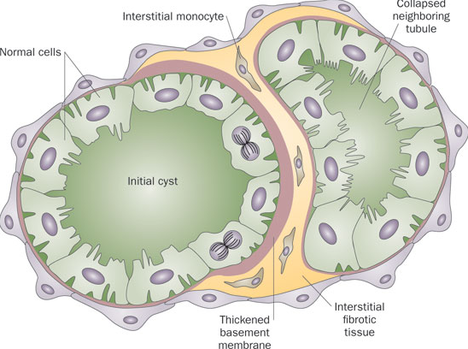
During development of kidney cysts, a tubule cell will divide repeatedly to form daughter cells that are not differentiated and thus have no specific function. The proliferation of these cells is directed by mitogens, which direct growth at a rate of ~5-6% each year [5]. These growing cells have altered growth responses, abnormal expression of proteins, and changes in polarity [6]. The epithelial cells which comprise the nascent cyst sense damage, and produce chemokines and cytokines that promote inflammation [7].
The cyst expansion compromises adjacent tubules and collapses capillaries, lymphatics, and larger arterioles and venules. Ultimately, noncystic nephrons are destroyed, leaving behind a network of cysts held in place by thick bands of fibrotic material [7].
Symptoms
The most prominent symptom of polycystic kidney disease is chronic pain in the back or sides, often with recurring headaches. The pain can be either mild or severe, temporary or recurrent [3].
Complications
- Urinary tract infections
- Hematuria-blood in the urine
- Liver and pancreatic cysts
- Abnormal heart valves
- High blood pressure
- Kidney stones
- Aneurysms-bulges in the walls of blood vessels within the brain [3]
Diagnosis
Diagnosis of polycystic kidney disease occurs typically through imaging studies, although conclusive diagnoses rely on molecular testing to demonstrate mutation within the causative gene [2]. Imaging is typically done using ultrasound, although computer tomography (CT) and magnetic resonance imaging (MRI) are also utilized in diagnosis. Furthermore, although genetic testing can be useful for identifying mutant copies of the gene, it cannot predict onset of disease or ultimate severity [3].
Treatment
Treatment often involves management of clinical manifestations, including:
When kidneys begin to fail, patients can seek out either dialysis or transplantation.
- Treatment of pain, including over-the-counter pain medication
- Treatment of hypertension involving ACE inhibitors or diet modification
- Cyst decompression
- Replacement of enlarged thoracic arteries [2].
When kidneys begin to fail, patients can seek out either dialysis or transplantation.
References
|
Site created by: Elizabeth Roeske Last Updated: 5.12.2014 University of Wisconsin-Madison: Genetics 564 |
